Glaucoma
Glaucoma is the second leading cause of blindness in the U.S. It most often occurs in people over age 40, although a congenital or infantile form of glaucoma exists. Glaucoma is a group of eye disorders that leads to progressive damage to the optic nerve eventually resulting in loss of vision. While it cannot be prevented, if diagnosed and treated early it can usually be controlled. That is why the American Optometric Association recommends an annual dilated eye examination for people at risk for glaucoma as a preventive eye care measure.
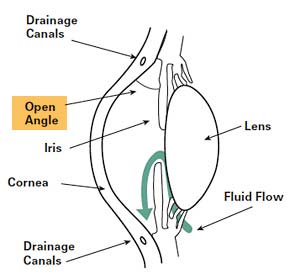
Open-Angle Glaucoma
 It is estimated that over two million Americans have some type of glaucoma and half of them do not know it. Ninety percent of glaucoma patients have open-angle glaucoma. Although it cannot be cured, it can usually be controlled. Vision loss may be minimized with early treatment.
It is estimated that over two million Americans have some type of glaucoma and half of them do not know it. Ninety percent of glaucoma patients have open-angle glaucoma. Although it cannot be cured, it can usually be controlled. Vision loss may be minimized with early treatment.
The eye receives its nourishment from a clear fluid that circulates inside the eye. This fluid must be constantly returned to the blood stream through the eye’s drainage canal, called the trabecular meshwork. In the case of open-angle glaucoma, something has gone wrong with the drainage canal. When the fluid cannot drain fast enough, pressure inside the eye begins to build.
This excess fluid pressure pushes against the delicate optic nerve that connects the eye to the brain. If the pressure remains too high for too long, irreversible vision loss can occur.
Symptoms

- In the early stages, there are no symptoms. There is no pain or outward sign of trouble.
- Mild aching in the eyes
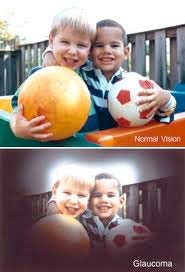
- Gradual loss of peripheral vision (the top, sides and bottom areas of vision)
- Seeing halos around lights
- Reduced visual acuity (especially at night, that is not correctable with glasses)
Who is at risk?
Glaucoma can occur in people of all races at any age. However, the likelihood of developing glaucoma increases if you:
- are African American
- have a relative with glaucoma
- are diabetic
- are very nearsighted
- are over 35 years of age
Diagnosing
Everyone should be checked for glaucoma at around age 35 and again at age 40. Those considered to be at higher risk, including those over the age of 60 should have their pressure checked every year or two.
Your doctor will use a tonometer to check your eye pressure. After applying numbing drops, the tonometer is gently pressed against the eye and its resistance is measured and recorded.
An ophthalmoscope will be used to examine the shape and color of your optic nerve. The ophthalmoscope magnifies and lights up the inside of the eye. If the optic nerve appears to be cupped or is not a healthy pink color, additional tests will be run.
Perimetry is a test that maps the field of vision. Looking straight ahead into a white, bowl-shaped area, you’ll indicate when you’re able to detect lights as they are brought into your field of vision. This map allows your doctor to see any pattern of visual changes caused by the early stages of glaucoma.
Gonioscopy is used to check whether the angle where the iris meets the cornea is open or closed. This helps determine if you have open-angle or narrow-angle glaucoma.
Treatment
To control glaucoma, your doctor will use one of three basic types of treatments: medications, laser surgery or filtration surgery. The goal of treatment is to lower the pressure in the eye.
1. Medications
Medications come in pill and eye drop form. They work by either slowing the production of fluid within the eye or by improving the flow through the drainage meshwork.
2. Laser Surgery
Argon Laser Trabeculoplasty and Selective Laser Trabeculoplasty surgery treat the drainage canal. Requiring only numbing eye drops, the laser beam is applied to the trabecular meshwork resulting in an improved rate of drainage. When laser surgery is successful, it may reduce the need for daily medications.
Endoscopic CycloPhotocoagulation (ECP) is another type of laser procedure. Instead of treating the drainage canal, it treats the ciliary body. Treating the ciliary body reduces the amount of fluid production thereby reducing the intra ocular pressure. ECP is most often performed along with cataract surgery as an outpatient procedure. The majority of patients having ECP reduce or eliminate their need to take glaucoma medications.
3. Filtration surgery
This procedure is performed when medications and/or laser surgery are unsuccessful in controlling eye pressure. During this microscopic procedure, a new drainage channel is created to allow fluid to drain from the eye.
Narrow-angle glaucoma (also called closed-angle glaucoma)
Narrow-angle glaucoma is much more rare and is very different from open-angle glaucoma in that eye pressure usually goes up very fast. This happens when the drainage canals get blocked or covered over. The iris gets pushed against the lens of the eye, shutting off the drainage angle. Sometimes the lens and the iris stick to each other. This results in pressure increasing suddenly, usually in one eye. There may be a feeling of fullness in the eye along with reddening, swelling and blurred vision.
Symptoms
 The onset of acute narrow-angle glaucoma is typically rapid, constituting an emergency. If not treated promptly, this glaucoma produces blindness in the affected eye in three to five days.
The onset of acute narrow-angle glaucoma is typically rapid, constituting an emergency. If not treated promptly, this glaucoma produces blindness in the affected eye in three to five days.
Symptoms may include:
- Inflammation and pain
- Pressure over the eye
- Some pupil dilation
- Cloudy cornea
- Blurring and decreased vision
- Extreme sensitivity to light
- Seeing halos around lights
- Nausea and/or vomiting
Causes
- Defect in the eye structure
- Anything that causes the pupil to dilate — dim lighting, dilation drops
- Certain oral or injected medications
- Blow to the eye
- Diabetes-related growth of abnormal blood vessels over the angle
Diagnosing Narrow-angle Glaucoma
Everyone should be checked for glaucoma at around age 35 and again at age 40. Those considered to be at higher risk for narrow-angle glaucoma, including those who are Asian, farsighted or over the age of 60, should have their pressure checked every year or two. Because of the rapid, potentially devastating results of narrow-angle glaucoma, you should seek medical treatment immediately if you experience any of the above symptoms.
Treatment
Laser iridotomy is a common treatment for narrow-angle glaucoma. During this procedure, a laser is used to create a small hole in the iris, restoring the flow of fluid to the front of the eye. In most patients, the iridotomy is placed in the upper portion of the iris under the upper eyelid, where it cannot be seen.
Filtration surgery is performed when medicines and/or laser surgery are unsuccessful in controlling eye pressure. During this microscopic procedure, a new drainage channel is created to allow fluid to drain from the eye.